Edwar Alvarez MD,1 Usman Khalid Farooq,2 David Alvarez MD,3 Andrea Iñiguez MD,4 Ghulam Qadir Fayyaz5
1,3,4Reconstructive and Aesthetic Plastic Surgery Service, 2Continental Basic Hospital. Latacunga-Ecuador, 2Department of Plastic Surgery / Mayo Burn Centre, KEMU, Mayo Hospital, Lahore, 5CLAPP Hospital, Lahore
Abstract
Introduction: Bleeding, during post-operative period is not only frustrating for the surgeon but may also lead to life threatening condition for the patient. Sometimes if uncontrolled or not managed adequately can lead to death of patient. It’s a worldwide problem as evident with articles from all over the world, especially dangerous in pediatric patients and more specifically cleft surgery patient post operatively.
Objective: The objective of the study was to determine an algorithm which can help in the management and prevention of postoperative bleeding cleft patients.
Methods: This paper presents the Red Code Algorithm, for pre, intra and postoperative management of cleft patients. The study was performed in different centers of Smile Train Foundation in Ecuador, Peru, Paraguay, Nicaragua and Morocco.
Results: We studied 864 primary and secondary cleft lip and palate surgeries, performed during one year by the same group of surgeons. In these 864 consecutive cases the Red Code Algorithm was applied. Forty-five patients (5.3%) presented more bleeding compared to the average of patients, and 2 cases (0.23%) required surgical re-intervention for hemostasis control. The control group had a total of 1243 patients, who had surgery by the same team before the introduction of the Red Code Algorithm. Of them, 113 cases (9.1%) presented more bleeding compared to the average, and 37 cases (2.97%) required surgical re-intervention to achieve hemostasis control.
Conclusion: This approach reduced the incidence of postoperative bleeding in all types of cleft surgeries.
Keywords | Red Code, Bleeding, Cleft surgery Received | 08-08-2020: Accepted | 02-10-2020 Corresponding Author: Edwar Alvarez MD
E-mail: edwaralvarezc@hotmail.com
Introduction
Bleeding during post-operative period is not only frustrating for the surgeon but may also lead to life threatening condition for the patient. He may even do revision surgery immediately to control the bleeding, which can be difficult to stop. Sometimes if uncontrolled or not managed adequately can lead to death of patient. It’s a worldwide problem as evident with articles from all over the world, especially dangerous in pediatric patients and more specifically cleft surgery patient post operatively.1
Another aspect is cost of treatment of patients. It increases many a fold due to not only the demand of medical personnel’s but also the operation theater items, gases and disposables Many studies have been done previously in this aspect but not many specifically for cleft lip and palate
patients. In Levy’s studies on cardiac surgery,6,8 it was determined that about 4.7% of their cases needed re- exploration because of bleeding. In Jerrold study on trauma and orthopedics, percentage decreased to 1.9% as comparison to Levy’s (RR, 0.44, 95% CI,0.22 to 0.90), after applying their red code which also decreased morbidity and mortality.8
Reviews on cleft surgeries reveal that about 13% of them, presented an abnormal bleeding, and about 4.8% needed re-intervention to control hemostasis.
Experience has taught us that in most cases, “normal” postoperative bleeding stops after applying digital pressure for few minutes but sometimes due to any circumstance the bleeding restarts hours after the end of the surgery. This situation may lead to a late diag- nosis and re-intervention with possible complica- tions. On the other hand, the opposite situation may also occur: the patient may be rushed into the opera- tive room to review bleeding under general anes- thesia, and once the patient is intubated no further bleeding appears. Sometimes the bleeding is tried to be controlled with pharmacological drugs as evidenced with Levy’s studies.8 This shows us that we don’t have a clear algorithm that allows us to decide either re-intervention without loss of time (negative false), or discharge positive false. So, this study is done to determine an algorithm which can be applied to the pediatric patients of primary and secondary cleft lip and palate interna-tionally for the better management in regard to the patient care.
Methods
It is a multicentric study performed from January 2019 to December 2019 for a period of one year in Ecuador, Peru, Paraguay, Nicaragua and Morocco, within each country Operation Smile Foundation and with the respective knowledge and approval of the corresponding medical directors, the Red Code, des- cribed below, was routinely applied for the preven- tion of postoperative bleeding in primary and secon- dary cleft lip and palate patients. 864 patients were included in the study and surgeries were performed by same group of surgeons. The results were compa- red with those from the same countries, from a period of three years, when the Red Code Algorithm was not yet applied. Following are the operational definitions.
Hemostatic Safety Bleeding (HSB)
For a “predictor» to know which volume of blood loss in a cleft surgery could leave the patient without enough coagulation factors, that the patient would need in the postoperative period if a major bleeding appeared. So, with this “predictor” we could define measures to control the loss of coagulation factors, and unnecessary transfusions, and revisions.4
Our study was able to define that cleft surgeries in patients whose intra-operative bleeding volume rea- ched 10% of their total volume, needed the use of preventive measures, such as pro-coagulant medica- tion, and others to avoid immediate surgical reviews and even blood products transfusions.
In our study we have adopted this value of 10% of the calculated total blood volume of each patient based on the HSI or Hemostatic Safety Index which, once reached, actives the Cleft Patient Surgery «RED CODE», setting in motion mechanisms focused on saving intraoperative coagulation factors, and elimi- nating false positives that confuse the diagnosis of persistent bleeding in the postoperative period.
Permitted Bleeding
This is the index that indicates the maximum amount of blood that a patient can lose until he reaches a minimum tolerable total blood volume. Once this value is exceeded the patient will need measures of blood replacement according to protocols; the Anes- thesia Mexican Association has developed a calcula- tor which, in an elective surgery, generally represents a value close to 20% of the patient calculated total blood volume.5
Alpha- and Beta-Adrenergic effect
Epinephrine acts in both α and β receptors causing vasoconstriction and vasodilation respectively. At high circulating concentrations α receptors cause vasoconstriction, an effect that is predominant for the first hour overcoming the beta effect. In the second hour, the low circulating levels of epinephrine pro- duce stimulation of β receptors. It produces therefore general vasodilatation from the second hour until its effects disappear at the third hour.11
Tranexamic acid
Tranexamic acid is an active hemostatic agent which can be administered orally and parenterally. It has effects similar to those of aminocaproic acid, but it is about 10 times more potent as an inhibitor of plas- minogen activation, reducing the dissolution of hemostatic fibrin by plasmin.
After an administration of 1300 mg of tranexamic acid, the maximum plasma concentrations are reached after 3 hours. Absolute oral bioavailability is appro- ximately 45%. A decrease in plasma levels is observed according to a triexponential equation, with a half-life of elimination of about two hours. After intravenous administration of 10 mg / kg, approximately 90% of the dose is eliminated in about 24 hours.11
In general, 1.4% of the patients presented adverse reactions such as nausea and vomiting, diarrhea, hypotension, dizziness, visual abnormalities and alte- rations of the retina. Venous and arterial thrombosis and thromboembolism have also been reported, as well as obstructions of the retinal artery and vein. Urethral obstructions have also been described occa- sionally due to formation of clots in patients with upper urinary tract hemorrhage.
Aminocaproic acid
Aminocaproic acid belongs to a class of medications called pro-hemostatic. It works by slowing the disin- tegration of blood clots. (MedlinePlus, 2010). It is used to control bleeding that occurs when blood clots dissolve too quickly. This type of bleeding can occur during or after surgery of the heart or liver, in people with certain bleeding disorders; in people with pros- tate, lung, stomach or cervix cancer and in pregnant women with abruptio placentae. Aminocaproic acid should not be used to treat bleeding that is not caused by rapid disintegration of a blood clot.11
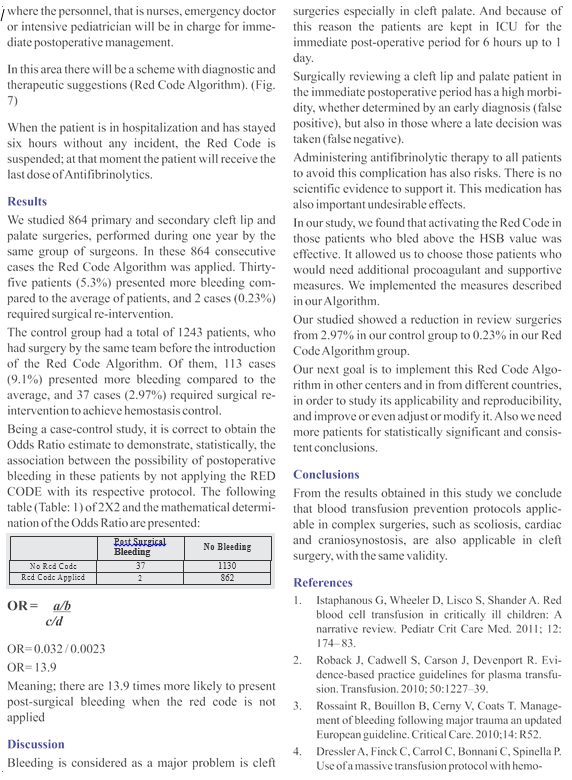
Red Code Algorithm
It is important to understand that not all surgeries have the same bleeding risk, for example the palate surgery is riskier due to vascularization, which is very rich. The lip repair has minor risk but it exists.
The bleeding prevention in cleft surgery will begin in the preoperative, and continue in intraoperative and postoperative phases.
Preoperative Phase
It consists of integral clinical evaluation to assess the presence of patients with bleeding risk. In this phase it is imperative the role of:
The Pediatrician. – They must specify clinical conditions involving coagulation disorders such as Von Willebrand disease, mild hemophilia A, conge- nital disorders of platelet function: Bernard Soulier syndrome, vascular disorders: Ehlher Danlos, Marfan syndrome, Wilms tumor, myelin and lymphoproli- ferative diseases, hypothyroidism, congenital heart disease.
The Anesthesiologist. – They will determine the Permitted Bleeding value of the patient, according to weight, the real hematocrit and the minimum value the patient can reach. This value is usually around 20% of the total blood volume. The Hemostatic Safety Bleeding value will be around 10% of this volume.
They will also determine as usual other parameters of importance relating to airway manage and difficult airway patient.
The Cleft Surgeon – In this phase, they will evaluate the extent, complexity, and the possible bloody areas of the surgery.
Intraoperative Phase
In this phase the whole teams work together to eva- luate the intra-operative bleeding.
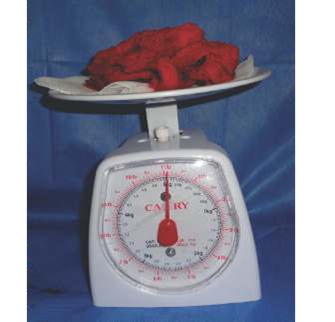
Auxiliary Nurse:- In order to assess the exact amount of blood loss, the Auxiliary Nurse will quan- tify the amount of blood collected in the suction container (having previously verified it was empty at the beginning of the surgical procedure) and in the gauzes and compresses used (counting them, kno- wing that one completely wet gauze contains 10cc of blood). They will also quantify the saline used for surgical irrigation when considering the liquid collec- ted in the suction container. In case the blood loss exceeds the previously defined HSB value (Hemo- static Safety Bleeding value) for that patient, the “Red Code” will be activated.
In order to quantify how much blood is contained in a gauze or compress, we have carried out field tests to define that value. We concluded that each square centimeter of gauze with four layers is impregnated with one gram of blood. (Fig. 1)


Scrub Nurse. – They must quantify the saline solution used during the surgery, and must also count the number of gauzes used (completely wet gauzes, as shown in (Fig. 3) in order to eventually determine the intra-operative blood loss. If the value exceeds the patient HSB, the RED CODE will be activated, and adequate treatment started according to our Red Code Algorithm.
Photographer- Photographic records of the cases will be examined. The purpose is to document the bleeding through pictures (the gauzes used and the blood collected in the suction container, and any other measure taken (flushing of the surgical field, bloody gastric content…)
Anesthesiology, Pediatrics, Nursing- Once the Red Code has been activated intra-operatively, the reasons for the bleeding shall be verified for quantification of that bleeding (recount of gauzes, suctioned blood, etc.) for definitive quantification.
Medication shall be initiated as indicated in the Red Code Algorithm: Dexamethasone, Tranexamic Acid and Ondansetron. Antibiotics in therapeutic dose should also be initiated.
Quantification of the bleeding will continue until the end of the surgery
Cleft Surgeon- The surgical team leader might assist the surgeon performing the surgery in assessing the case, identifying the reasons for the bleeding and controlling it. They will follow the Red Code Algo- rithm.
At the end of the surgery, the surgeon should flush with saline the oral and nasal cavity to remove the clots, and aspirate the pharynx and gastric contents (Fig. 4). If this procedure is not done, it could mislead us, because it might be from previous intra-operative bleeding or be new.
Scrub Nurse. – They must quantify the saline solution used during the surgery, and must also count the number of gauzes used (completely wet gauzes, as shown in (Fig. 3) in order to eventually determine the intra-operative blood loss. If the value exceeds the patient HSB, the RED CODE will be activated, and adequate treatment started according to our Red Code Algorithm.
Photographer- Photographic records of the cases will be examined. The purpose is to document the bleeding through pictures (the gauzes used and the blood collected in the suction container, and any other measure taken (flushing of the surgical field, bloody gastric content…)
Anesthesiology, Pediatrics, Nursing- Once the Red
Code has been activated intra-operatively, the reasons for the bleeding shall be verified for quantification of that bleeding (recount of gauzes, suctioned blood, etc.) for definitive quantification.
Medication shall be initiated as indicated in the
Red Code Algorithm: Dexamethasone, Tranexamic Acid and Ondansetron. Antibiotics in therapeutic dose should also be initiated.
Quantification of the bleeding will continue until the
end of the surgery
Cleft Surgeon- The surgical team leader might assist the surgeon performing the surgery in assessing the case, identifying the reasons for the bleeding and controlling it. They will follow the Red Code Algo- rithm.
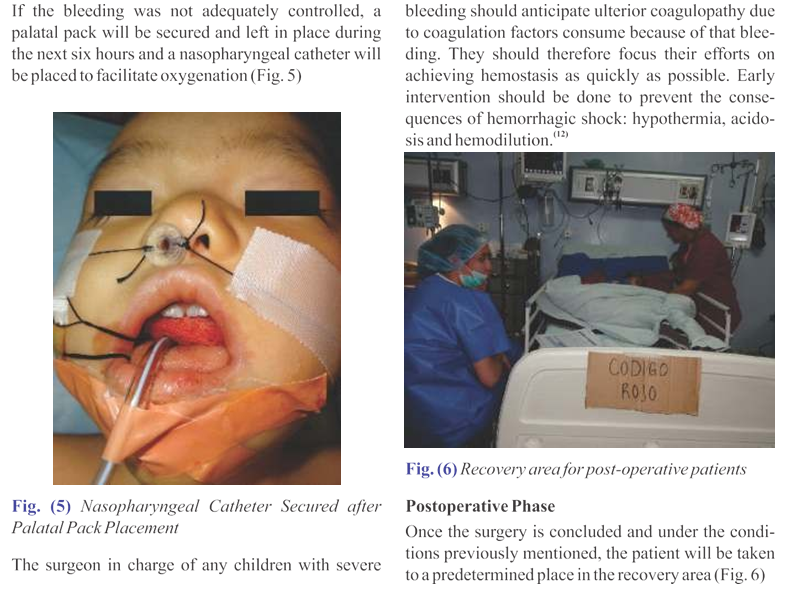
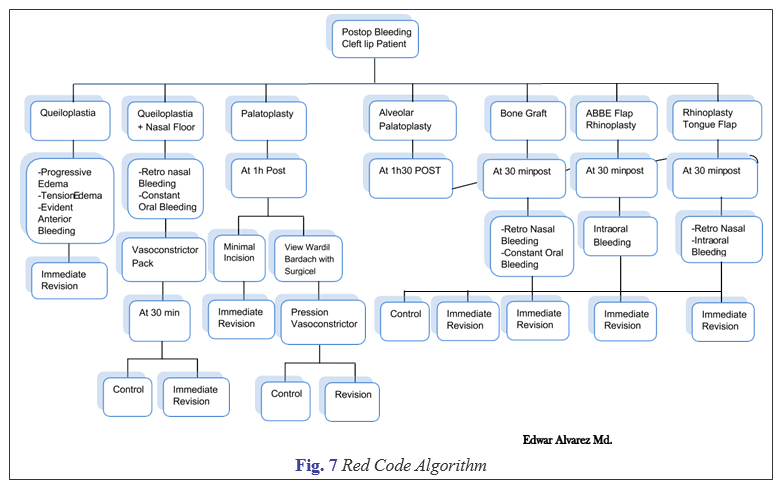
At the end of the surgery, the surgeon should flush with saline the oral and nasal cavity to remove the clots, and aspirate the pharynx and gastric contents (Fig. 4). If this procedure is not done, it could mislead us, because it might be from previous intra-operative bleeding or be new.